
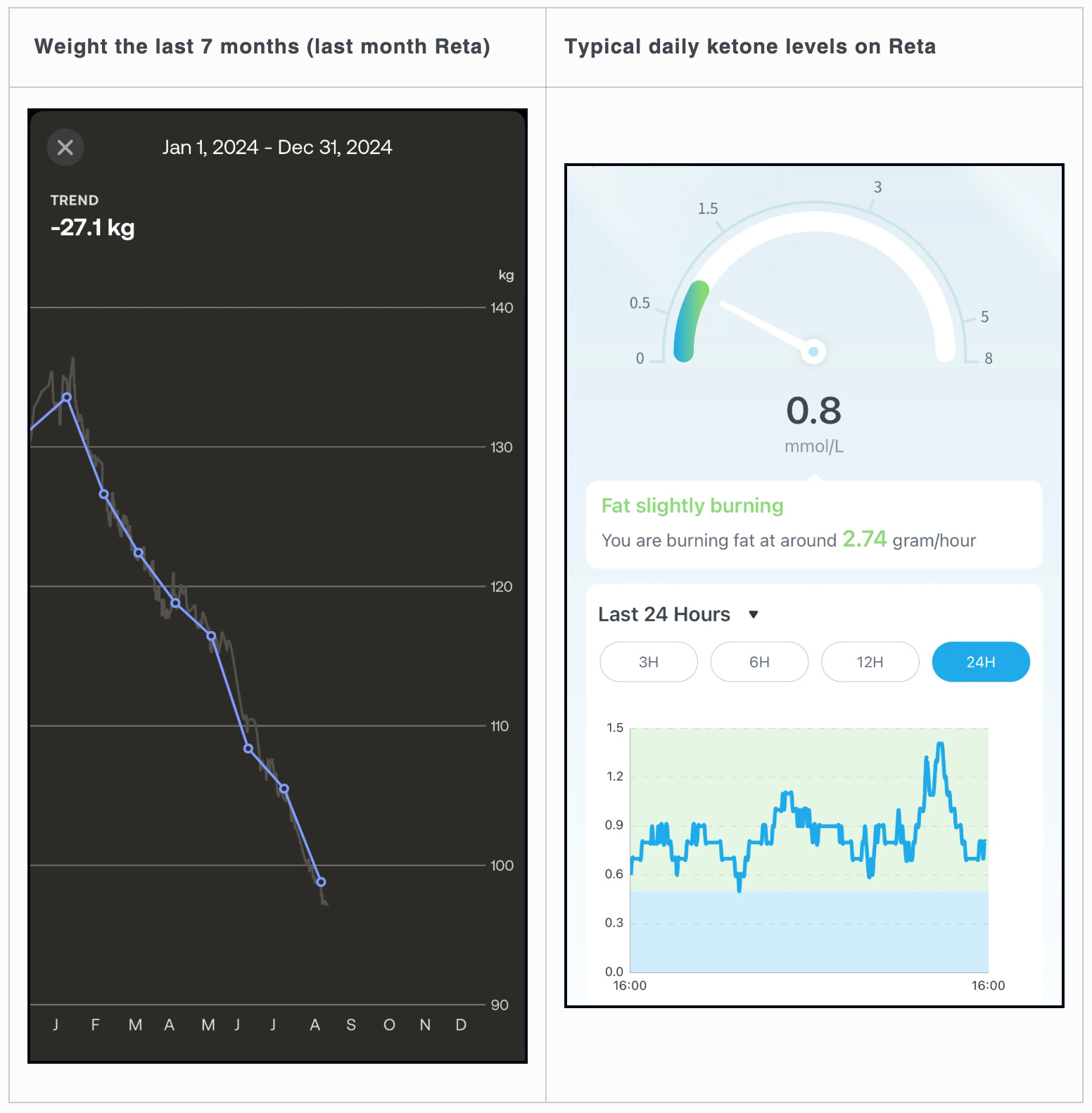
Losing 17 lbs in a month on Retatrutide: Much more energy than Tirzepatide

NOTE: This is not medical advice or advice of any kind. This is a personal research document.
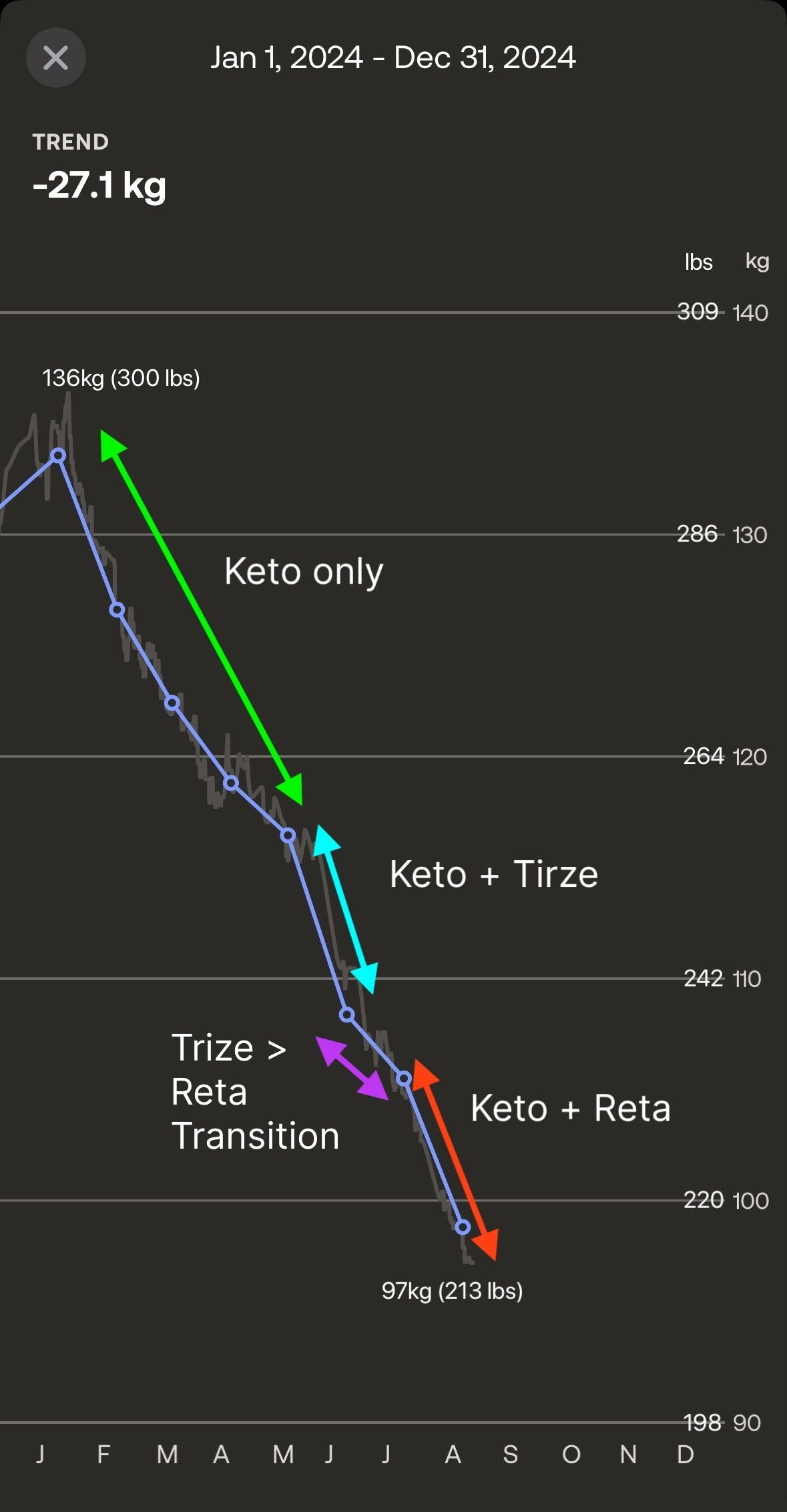
After trying the new "3rd generation" GLP-1, Retatrutide, for 2 months, I find it much more effective than Tirzepatide and with less side effects (namely fatigue).
My weight-loss has been about the same, if not slightly quicker, but more importantly, my energy levels are much higher, and most interestingly, my blood ketone baseline has been higher.
On Tirzepatide, while effective, I would get fatigued if I didn't carefully manage my energy state by doing things like drinking extra water, making sure I ate on time, and supplementing with exogenous ketones.
I am sharing all the details on exactly where and how Retatrutide was used in this journey, but first a bit of background on Retatrutide...
What is Retatrutide?
The "GLP-1" class of peptides has a few different types of peptides:
Gen 1 - Semaglutide, also known as Ozempic or WeGovy, is a single mechanism peptide. This is a GLP-1 (glucagon-like peptide-1) receptor agonist. It works by mimicking the effects of GLP-1, a hormone that promotes insulin release, reduces appetite, slows gastric emptying, and regulates blood sugar.
Gen 2 - Tirzepatide, also known as Mounjaro, is a double mechanism peptide. It is both a GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptor agonist. GIP enhances insulin secretion and may play a role in lipid metabolism, synergistically with GLP-1 effects.
Gen 3 - Retatrutide is the new peptide that is still undergoing phase 3 (final) clinical trials with the FDA. This is a triple agonist targeting GLP-1, GIP, and glucagon receptors. Glucagon receptor activation can enhance energy expenditure and further promote fat loss. This last point is key when it comes to increasing blood ketone levels.
The Hunger Hormones - Insulin and Glucagon
Insulin is the hormone that facilitates the entry of glucose into our cells, where it is used for energy. It also signals to the liver to convert glucose into glycogen for short term storage, or fat for long term storage.
When there is a lot of insulin circulating in the blood, one feels full, bloated, or even nauseous. If you've ever eaten way to much, you are familiar with this feeling.
The GLP1 and GIP mechanisms in Semaglutide and Tirzepatide encourage a stronger insulin response to blood glucose, increasing the insulin response to glucose entering the blood stream, and increasing the sensitivity of our cells to absorb glucose.
This is the main mechanism of weight-loss for these two peptides, use glucose more effectively and make one feel full quicker.
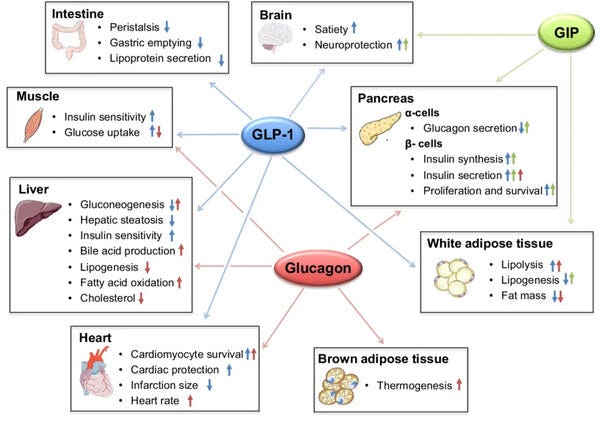
Glucagon is the other hormone that helps our cells get energy. When insulin levels fall in response to a lack of blood sugar, the pancreas secretes Glucagon, which signals to the liver to do the opposite of insulin: mobilize the stored glycogen for energy, and when that runs out, activate the long term fat storage as an energy source.
This is the mechanism that activates ketosis! A shortage of glucose (carbs) triggers Glucagon to signal to the liver to convert stored body fat into ketones, to be used as a backup energy source.
One can see why adding this 3rd mechanism would be very beneficial for fat loss, as not only is insulin being more effective, but glucagon is being stimulated as well.
As I was studying the mechanisms of ketosis and the glucagon/insulin relationship, I was quite excited to come across Retatrutide's Glucagon agonist mechanism, as I hypothesized it would enable an easier and more consistent ketogenic state, which would also mitigate the low energy issues with Tirzepatide.
Results of the Phase 2 Trial
Retatrutide is patented by Eli Lilly, who has completed a phase 2 clinical trial with the FDA: https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
I read through the entire trial to see if I could confirm my hypothesis that the Glucagon agonist would increase weight-loss and induce ketosis, as well as study any adverse effects.
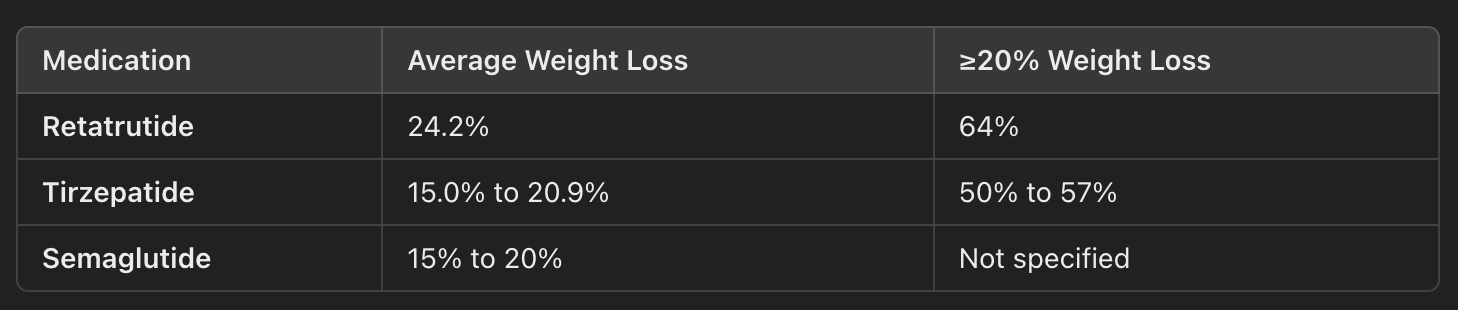
The results on weight loss seemed quite significant, a roughly 20% increase vs. Tirzepatide or Semaglutide. Unfortunately the study did not seem to measure ketone levels and gave no indications around ketosis.
Since it is a relatively new and untested compound, I wanted to check if there were new side effects vs. existing GLP1s peptides.
I studied the adverse event table from the trial: https://www.nejm.org/doi/full/10.1056/NEJMoa2301972#ap2
Most concerning was 1 death and 13 serious adverse events, out of 337 total. Ok well the 1 death was from drowning and concluded to be unrelated. There were several serious cardiac events however, including among the placebo group. Ok good time to revisit the selection criteria for the study:

Ok, so the participants had to be extremely obese, or obese with a pre-existing heart condition. Additionally the average age was around 48, so skewed to the older side. Given the selection criteria and sample size of 337 split into 7 groups, I personally do not find the data to be conclusive around whether the cardiac incidents were related to Retatrutide or not.
Additionally, there were 19 reports of Cardiac Arrhythmia out of the 337 participants. Given the participants were selected with pre-existing cardiovascular conditions, how much of an impact did Retatrutide have on this effect?

Again, the smaller sample size skews the data a bit, but we can see the average rate of arrhythmia in the 1mg-4mg groups is roughly the same or slightly higher than placebo. However in the higher dose groups, 8mg-12mg, the Arrhythmia incidents seemed to increase substantially. Ok, so this is something to keep an eye on.
Hypothesis: some of the causes of arrhythmia include electrolyte shortage, low blood sugar, and glycogen shortage. Given that Insulin moves glucose out of your blood stream, and Glucagon mobilizes your glycogen reserves, its quite possible that this is causing a shortage of glucose or glycogen energy shortage for the heart at higher doses. Finding ways to mitigate this would be interesting, but probably something one would want to test in rats first.
EDIT: The above hypothesis is probably incorrect.
It turns out that Glucagon, among other things, directly stimulates the heart, and is even used in emergency room contexts to get the heart going again. It seems likely this is the cause of increased heart rate and arrhythmia at higher doses.
To monitor for potential Arrhythmia, things I watch out for:
Increased heart rate, especially resting heart rate, lowered HRV, increased blood pressure, heart palpitations
Getting dizzy easily during physical activity
Shortness of breath, chest pain or discomfort, fainting
Heart monitoring devices that can check for arrhythmia
Ultimately it probably makes sense to stay away from higher doses until it is better studied.
What about other adverse reactions?
Hypoglycemia - "No cases of clinically significant hypoglycemia." Regardless I personally always watch for mild hypoglycemia, especially when starting or increasing doses of GLP1s, as the increased insulin levels can remove blood sugar quickly.
Pancreatitis - as Glucagon is secreted by the pancreas, this may be putting extra strain on the pancreas and is something I wanted to watch out for. 1 case of pancreatitis in the trial.
abdominal pain, characteristic of acute pancreatitis (that is, epigastric pain radiating to the back, often associated with nausea and vomiting)
serum amylase (total, pancreatic, or both) and/or lipase ≥3X ULN
Liver - as all 3 mechanisms affect the liver, I wanted to keep an eye on this as well.
"Transient increases in alanine aminotransferase (ALT) levels to more than 3 times the upper limit of the normal range occurred in 1% of the participants who received retatrutide"
Heart
The heart rate increased in a dose-dependent manner with retatrutide up to 24 weeks and then declined thereafter
Avg heart rate increase was 10bps, compared to 3bps on Tirzepatide
After digesting all this, I was comfortable with replacing Tirzepatide with Retatrutide and seeing if it would indeed increase my blood ketones and overall energy.
Starting on Retatrutide
For these GLP1s, I personally prefer to dose daily to reduce any "swings" in effectiveness and have more fine grained control over dosing. I started this after trying Tirzepatide on weekly dose and finding that I'd rebound at the end of the week due to the ~5 day half life.
For my GLP1 doses, I will include the daily (weekly) dose in that format.
For reference, the dose schedule for Tirzepatide vs. the dose schedule used in the Retatrutide trial

Since I was already on Tirzepatide 2mg daily (14mg weekly), I hypothesized that I would already have a tolerance to the first 2 mechanisms of Retatrutide but no tolerance to the 3rd mechanism. So I designed a transition protocol for myself to switch over for a month.
First I wanted to test if I would be a hyper responder to Retatrutide or be sensitive to any side effects, so I did a quick ramp up in small doses, aiming for a weekly equivalent of about 4mg. At the same time I dialed down tirzepatide from 2mg daily to 1.5mg daily (10.5mg weekly):

No adverse affects, so I ramped down Tirzepatide to 1mg daily (7mg weekly), and increased Retatrutide to 1mg daily (7mg weekly).
That week I was HUNGRY. Retatrutide works a bit differently, and apparently most people experience an INCREASE in hunger when they first start it. However I got full and stayed full much quicker than even on Tirzepatitide, and reports I've read from others say similarly.
After two weeks, I started to feel the appetite suppressant effect kick in, so I increased my Retatrutide dose to 1.5mg daily (10.5mg weekly) and discontinued Tirzepatide entirely. This dose has been the same for the rest of this dataset.
Since I've been in this stable state with Retatrutide, I noticed a very clear energy increase vs. Tirzepatide.
The appetite suppressant effect is there to the point where I would forget to have a meal. Supplementing with protein powder and carrying around a bunch of Chomps beef jerky has been critical to hitting my protein target and maintaining muscle.
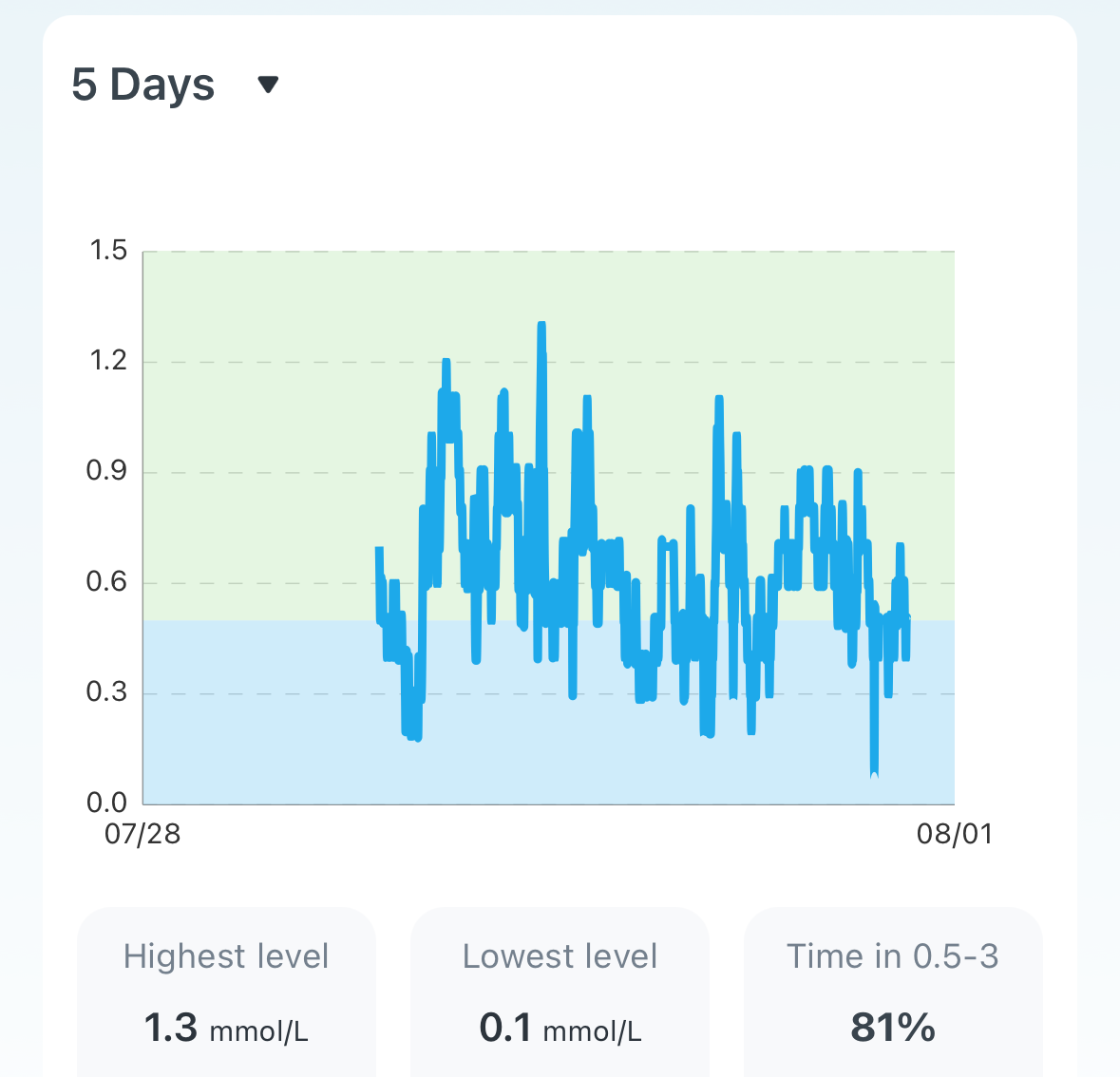
If I missed a meal on Tirzepatide, I would get really fatigued and cranky, not so on Retatrutide. And I was able to confirm using my Continuous Ketone Monitor that indeed, my average ketone levels were higher! On Tirzepatitide I would typically hover around 0.5 mmol/L, on Retatruide 1-1.5 mmol/L was more typical.
After the transition period, weight loss accelerated again, resulting in a 17 pound loss in a month.
Adverse effects
Surprisingly very little negative effects! I did not notice any change in my RHR, I have no more fatigue, and I do not experience any of the other negative effects. I do typically have a minor hypoglycemic event when I increase the dose, as I do on other GLP1s, which I pre-empt by taking exogenous ketones and having some protein handy. (the proper way to treat this is with sugar water, but I prefer not to spike my glucose)
EDIT: As I increased my dose up to 10mg-14mg weekly I started to notice the effects of Arrhythmia. I ended up discontinuing it while I reset my tolerance and intend to return to it.
Conclusion
As I have validated that Retatrutide meets all my goals of weight loss, high energy, and minimal side effects, I plan to continue using Retatrutide until my body fat target has been met. Tirzepatide was great too, but managing the fatigue was an ongoing effort.
It is important to note that throughout this entire experiment, I have maintained a mostly carnivore diet of meat, eggs, dairy, and a bit of green vegetables. My protein target is 200g/day and my carb target is 0g/day. I also make sure to intake electrolytes and other supplements as one would on a typical keto diet. I also exercise at least 3x per week.
Please note that nothing in this post is advice of any sort. Its especially definitely not medical advice. This is sharing my own research and experiences. Don't do anything I do.
Follow me on Twitter for more bio-hacking experiments: https://x.com/_TomHoward
EDIT: PS. Prudent Comment

How are you acquiring retatrutide?